מתיחת בטן
Abdominoplasty
נבדק על ידי ד"ר הלן הוינס, MRCGPעודכן לאחרונה על ידי ד"ר ג'קלין פיין, FRCGPעודכן לאחרונה 24 Mar 2016
עומד בהנחיות העריכה של Patient
- הורדהורד
- שתף
- Language
- דיון
- גרסת שמע
- הוסף למקורות מועדפים בגוגל
דף זה נשמר בארכיון.
זה לא נבדק לאחרונה ואינו מעודכן. קישורים חיצוניים והפניות עשויים לא לפעול יותר.
In this procedure excess skin and fat can be removed, abdominal contours and scars improved, and the muscles tightened.
במבט חטוף
מתיחת בטן היא הליך כירורגי להסרת עור ושומן עודפים מהבטן.
ישנם סוגים שונים של מתיחת בטן, כולל סטנדרטית, מיני, מורחבת ואנדוסקופית.
ההליך בדרך כלל משאיר צלקת ארוכה על פני הבטן התחתונה, לפעמים עם צלקת סביב הטבור.
Numbness and swelling in the lower abdomen are common after surgery.
התוצאות הטובות ביותר נראות אצל אנשים במשקל בריא.
יהיה עליך להפסיק לקחת את הגלולה למניעת הריון ולהפסיק לעשן לפני הניתוח כדי להפחית סיכונים.

This leaflet is provided by the British Association of Aesthetic Plastic Surgeons, the professional body responsible for the advancement of education and safety in aesthetic plastic surgery.
This is also called an abdominoplasty or tummy tuck. Different combinations are combined in the various procedures.
The standard abdominoplasty
Standard abdominoplasty
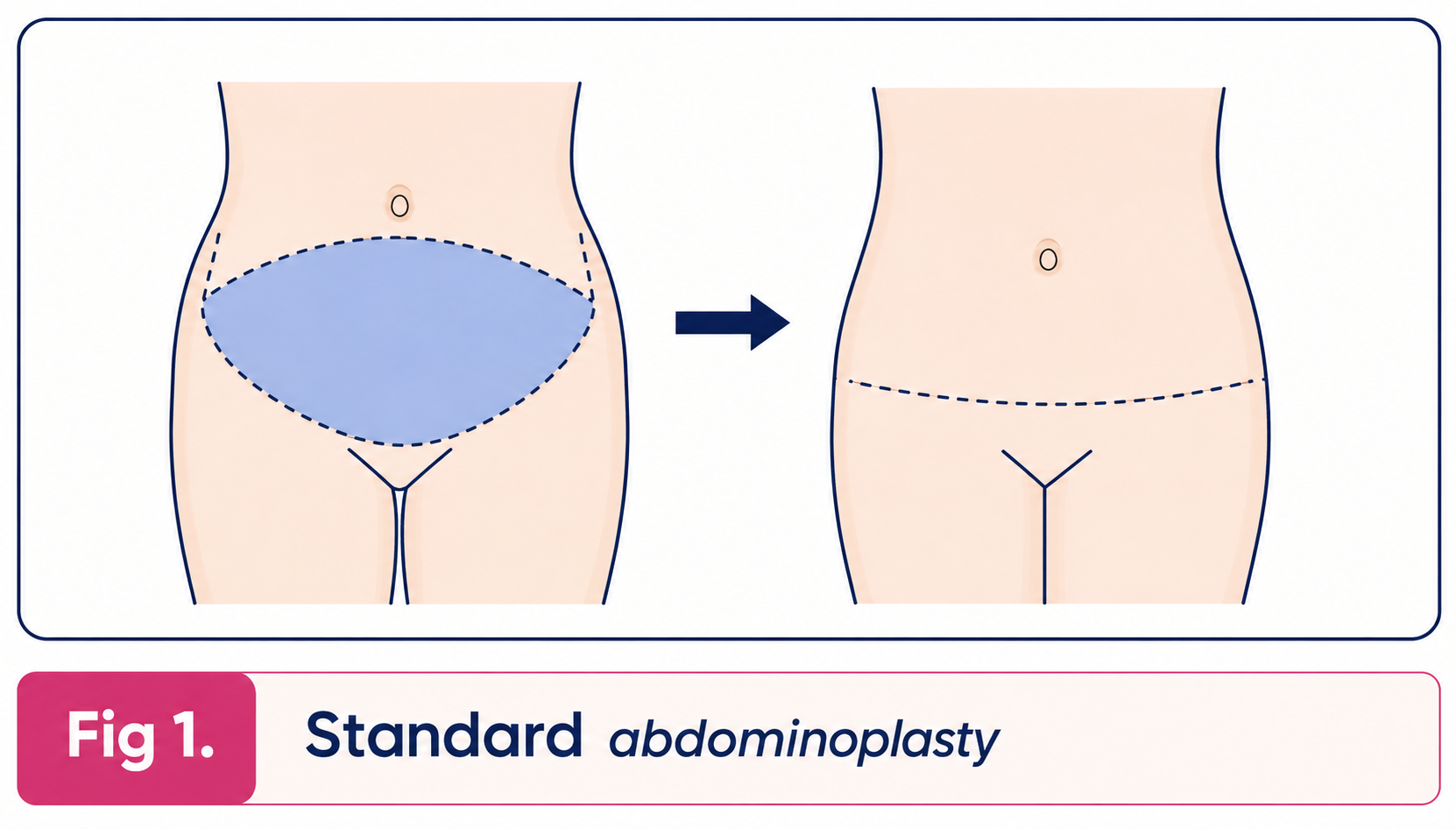
The excess skin and fat of the abdominal wall between the pubic area and the umbilicus (navel) is removed leaving the umbilicus in place. The skin of the abdominal wall at the level of the umbilicus is then drawn down to suture it at the pubic level. The patient is left with a long, usually curved scar across the lower part of the abdominal wall at the level of the pubic hair. There is also a scar around the umbilicus. Any looseness of the muscles of the abdominal wall or hernia is repaired at the same time.
Liposuction may be carried out during this procedure to thin the abdominal wall, or as a separate procedure either before or after the abdominoplasty.
Mini abdominoplasty
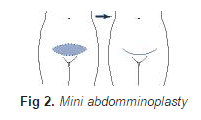
In the mini-abdominoplasty surplus skin below the umbilicus is removed leaving a low abdominal scar at the level of the pubic hair. The umbilicus is not disturbed but liposuction is usually carried out at the same time as the procedure to reduce the thickness of fat in the abdominal wall and any laxity or hernia of the abdominal wall is repaired at the same time.
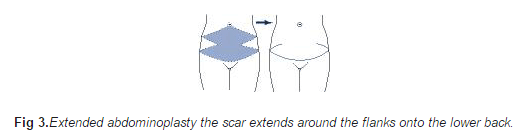
In the extended abdominoplasty surplus skin and fat of the loins and back are also removed so that the scar extends around the flanks on to the lower back.
Extended abdominoplasty
The endoscopic abdominoplasty is used to tighten the muscles of the abdominal wall to give a better contour and is carried out through a short transverse incision above the pubic hair. Skin is not removed but liposuction can be carried out at the same time.
The apronectomy is a modification of the mini-abdominoplasty for patients who have a large excess of skin and fat hanging down over the pubic area. In this procedure only the surplus skin and are removed. The scar is long and transverse extending from one side of the apron to the other.
Modifications to the abdominoplasty skin excision are made when the patient has particular problems associated with scars from previous operations.
An alternative procedure which should always be considered instead of many of the above is liposuction on its own. This reduces fat and causes just a little retraction of the skin.
Who is a candidate?
Anyone who has abdominal skin and fat may be a candidate. With women the problem is usually caused by pregnancy, but is greatly aggravated by בהרזיה. The muscles of the abdominal wall may be weakened by pregnancy and actually pulled apart in the middle (divarification of recti). Men are similarly affected by weight loss. Stretch marks (striae) are simply the scars which are left after extreme stretching of the skin. They are usually most apparent on the lower part of the abdominal wall. There is no specific treatment for these stretch marks, but many of them are excised in an abdominal reduction and those that are left are tightened making them look less obvious.
Patients that are unable to tighten the abdominal wall skin with exercise or wish to achieve a smoother flatter abdomen will also benefit.
What are the consequences?
The patient is left with noticeable scars. The main scar runs transversely across the lower part of the abdomen (see illustrations above) and in a standard abdominal reduction there will be a scar around the umbilicus. Other or different scars may be left where the patient has particular individual problems. Some patients make better scars than others and in any case all scars are red initially. It is essential that the patient understands where these scars will be and should discuss them with the surgeon. Although we try to hide them beneath underwear and swimwear, fashions can change making previously covered scars visible.
There is numbness in the lower part of the abdominal wall after surgery. This is usually temporary but could be permanent. Swelling above the scar is usually present due to a collection of tissue fluid which normally drains to the groin. This swelling or oedema settles within a few months.
What are the limitations?
The skin is usually tightened downwards and this does not tighten the waist. If this is desired then one can consider removing skin vertically, but one should bear in mind that vertical scars of the abdomen are less good. The tissue of the abdominal wall is generally fatter than the groin and if liposuction is not carried out a fatty bulge may remain above the scar.
The beneficial effects of the operation will last well. However, the effects will be maintained better if the patient keeps exercising the muscles and the weight steady. A further pregnancy will of course stretch the skin again, although probably not to the same degree.
מהם הסיכונים?
The standard abdominoplasty is a large procedure requiring two to four days of hospitalisation. Drains are removed when they stop draining blood and serum a few days after the procedure. This fluid can reaccumulate after the drains are removed requiring drainage or aspiration.
Healing can be slow particularly in the tighter central part of the wound and sometimes dressings are needed for a few weeks. This is more common in patients who are overweight ו who smoke. This tends to leave more obvious scars which are tethered - these can be revised.
Secondary procedures are sometimes carried out to tidy up the results and will involve scar revision and limited liposuction. Displacement of the umbilicus to one side has been over-publicised and is rare. פקקת ורידים עמוקים ו pulmonary embolus are rare complications of any operation, including this one.
What would you need to do before the operation?
If you are overweight you would be well advised to diet as best results are obtained in people who are the correct weight for their height. If you are taking the contraceptive pill you should stop doing so for six weeks before surgery and use an alternative method in order to reduce the risk of thrombosis. If you smoke there is a greater risk of chest infection and in particular healing of the abdominal wound is less good.
What you should expect at the time of the operation
You will need to be in hospital for one to three days. When you wake up for your operation it is likely that you will be having a transfusion of salt solution. This is quite normal and is to provide you with fluid you need whilst you are not drinking. You are likely to have drainage tubes coming out of each side of the lower abdomen which are there to drain any collection of blood or serum. You can expect some moderately severe pain for which you will be given painkilling tablets or injections. You will be asked to keep your knees and hips bent to take the strain off your stitches.
Recuperation
Overactivity in the early days reduces healing and increases fluid accumulation. Light activities are comfortable in 10 to 20 days. Sports will not be possible for about 6 weeks particularly when the muscles have been strengthened with sutures. A corset is usually helpful to reduce the swelling and improve comfort in the first month.
Content used with permission from the British Association of Aesthetic Plastic Surgeons website: Tummy Tuck (Abdominoplasty). Copyright for this leaflet is with the BAAPS.
הבהרה
This leaflet is designed to supply useful information but is not to be regarded as advice specific to any particular case. It does not replace the need for a thorough consultation and all prospective patients should seek the advice of a suitably qualified medical practitioner. The BAAPS accepts no liability for any decision taken by the reader in respect of the treatment they decide to undertake.
בחירות המטופלים עבור Other surgery and procedures

ניתוחים ופרוצדורות
וסקטומיה
Vasectomy is a a form of birth control where a man undergoes a small operation to cut the end of the vas deferens tube. This is the tube that takes sperm from the testicles (testes) to the penis. Sperm are made in the testes. Once the vas deferens is cut, sperm can no longer get into the semen that comes out (is ejaculated) during sexual intercourse. Vasectomy is very reliable - but not quite 100%. Even after a successful operation about 1 in 2,500 men who have had a vasectomy will become fertile again at some point in the future. This is because, rarely, the two ends of the cut vas deferens re-unite over time.
מאת ד"ר פיליפה וינסנט, MRCGP

ניתוחים ופרוצדורות
ניקוזים כירורגיים
ניקוז כירורגי הוא צינור פלסטיק קטן שמשמש לפעמים לאחר ניתוח. הוא מוכנס לתוך הגוף במהלך הניתוח על ידי הרופא ויבלט מחוץ לגוף עד שיוסר, בדרך כלל כמה ימים לאחר מכן. הוא מחובר לשקית פלסטיק קטנה שאוספת כל נוזל או אוויר שנוקזו מהמקום שבו בוצע הניתוח. לא כל הניתוחים דורשים ניקוז: המנתח שלך ייעץ לך אם יש צורך בכך.
מאת ד"ר רייצ'ל הדסון, MRCGP
שאלות נפוצות
מהי אפרונקטומיה, וכיצד היא שונה מהליכים אחרים של מתיחת בטן?
אפרונקטומיה היא סוג ספציפי של ניתוח מתיחת בטן המיועד למטופלים עם עודף משמעותי של עור ושומן התלויים מעל אזור הערווה, ולעיתים מכונים 'סינר'. בניגוד לכמה הליכים אחרים, הוא מתמקד אך ורק בהסרת העור והשומן העודפים הללו, ומשאיר צלקת ארוכה ורוחבית מצד אחד של הסינר לצד השני. הוא אינו כולל מיקום מחדש של הטבור או הידוק שרירים נרחב כמו שמתיחת בטן סטנדרטית עשויה לכלול.
האם ניתוח מתיחת בטן יכול להסיר לחלוטין את כל סימני המתיחה שלי?
ניתוח מתיחת בטן מתמקד בעיקר בהסרת עור ושומן עודפים. בעוד שסימני מתיחה רבים, במיוחד אלו שבחלק התחתון של דופן הבטן, עשויים להיות מוסרים יחד עם העור, חלקם עשויים להישאר. סימני המתיחה הנותרים יתהדקו עקב הקטנת העור, מה שיכול לגרום להם להיראות פחות בולטים, אך אין טיפול ספציפי לסימני המתיחה עצמם.
האם ניתוח מתיחת בטן יעזור לי להשיג מותניים צרים יותר?
באופן כללי, ניתוח מתיחת בטן בעיקר מהדק את העור כלפי מטה על הבטן, מה שבדרך כלל לא מהדק את המותניים. אם הידוק המותניים הוא מטרה ספציפית, ייתכן שיהיה צורך לשקול גישות חלופיות, כמו הסרת עור בצורה אנכית. עם זאת, חשוב לציין כי צלקות בטן אנכיות נוטות להיות פחות אסתטיות מצלקות אופקיות.
כמה זמן אחווה חוסר תחושה לאחר הניתוח?
תחושת נימול בחלק התחתון של דופן הבטן היא תופעה שכיחה לאחר ניתוח מתיחת בטן. מצב זה הוא בדרך כלל זמני, כלומר הוא אמור להיעלם עם הזמן. עם זאת, במקרים מסוימים, תחושת הנימול עלולה להפוך לקבועה.
מה אני יכול לעשות כדי להבטיח את התוצאות הטובות ביותר לטווח ארוך מהניתוח שלי לעיצוב הבטן?
כדי לשמור בצורה הטובה ביותר על ההשפעות המועילות של ניתוח מתיחת בטן, חשוב להמשיך לתרגל את שרירי הבטן ולשמור על משקל יציב. בעוד שהשפעות ההליך בדרך כלל נמשכות, תנודות משמעותיות במשקל או הריונות נוספים יכולים למתוח את העור שוב, אם כי ככל הנראה לא באותה מידה כמו קודם.
What is the typical hospital stay for a standard abdominoplasty?
ניתוח מתיחת בטן סטנדרטי נחשב להליך כירורגי משמעותי. מטופלים יכולים לצפות לאשפוז של יומיים עד ארבעה ימים לאחר הניתוח.
קריאה נוספת והפניות
- Calle EE, Rodriguez C, Walker-Thurmond K, et al; Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003 Apr 24;348(17):1625-38.
- Flegal KM, Kit BK, Orpana H, et al; Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013 Jan 2;309(1):71-82. doi: 10.1001/jama.2012.113905.
- Obesity in the UK: A psychological perspective; British Psychological Society, 2011
- Childhood overweight and obesity; World Health Organization
- Oude Luttikhuis H, Baur L, Jansen H, et al; Interventions for treating obesity in children. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001872. doi: 10.1002/14651858.CD001872.pub2.
- MEND; (Mind, Exercise, Nutrition ... Do it!)
- Position statement: Childhood obesity; Royal College of Paediatrics and Child Health, 2012
- Hsia DS, Fallon SC, Brandt ML; Adolescent bariatric surgery. Arch Pediatr Adolesc Med. 2012 Aug;166(8):757-66. doi: 10.1001/archpediatrics.2012.1011.
- Sjostrom L; Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013 Mar;273(3):219-34. doi: 10.1111/joim.12012. Epub 2013 Feb 8.
- Healthy lives, healthy people. A call to action on obesity in England; Dept of Health, 13 October 2011
- Reducing obesity and improving diet: Policy; Dept of Health, March 2013
- Body Mass Index (BMI) charts for girls and boys age 2-18; Royal College of Paediatrics and Child Health and Dept of Health
- Colquitt JL, Pickett K, Loveman E, et al; Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014 Aug 8;8:CD003641. doi: 10.1002/14651858.CD003641.pub4.
- Arterburn DE, Courcoulas AP; Bariatric surgery for obesity and metabolic conditions in adults. BMJ. 2014 Aug 27;349:g3961. doi: 10.1136/bmj.g3961.
- Obese, overweight with risk factors: liraglutide (Saxenda); NICE Evidence Summary, June 2017
- Hafekost K, Lawrence D, Mitrou F, et al; Tackling overweight and obesity: does the public health message match the science? BMC Med. 2013 Feb 18;11:41. doi: 10.1186/1741-7015-11-41.
- About Obesity: Body Mass Index; MEND - Mytime Active
- Yeh JS, Kushner RF, Schiff GD; Obesity and Management of Weight Loss. N Engl J Med. 2016 Sep 22;375(12):1187-9. doi: 10.1056/NEJMclde1515935.
אודות המחברצפה בפרופיל המלא

Dr Jacqueline Payne, FRCGP
רופא כללי, מחבר רפואי
MB, BS, DFFP, DRCOG, FRCGP
ג'קלין הייתה רופאת משפחה בקנדל, קומבריה במשך 25 שנים, שם היא הכשירה רופאים צעירים עבור ה-RCGP והייתה רופאה מדריכה עבור ה-FSRH.
אודות המבקרצפה בפרופיל המלא

Dr Helen Huins, MRCGP
רופא כללי, מחבר רפואי
MB, BS, Lond, DCH, DRCOG, MRCGP, JCPTGP, DFFP
Helen qualified at Guy’s Hospital in 1989 and left London in 1990 to settle in the countryside.
היסטוריית המאמר
המידע בעמוד זה נכתב ונבדק על ידי קלינאים מוסמכים.
המאמר זמין גם ב אנגלית, גרמנית, ספרדית, צרפתית, איטלקית, פורטוגזית, הינדי, עברית, ערבית, and שוודית.
24 Mar 2016 | הגרסה האחרונה

שאלו, שתפו, התחברו.
עיין בדיונים, שאל שאלות ושתף חוויות במאות נושאים בריאותיים.

מרגיש לא טוב?
הערך את הסימפטומים שלך באינטרנט בחינם
הירשמו לניוזלטר של פיישנט
המנה השבועית שלך של עצות בריאות ברורות ואמינות - נכתבה כדי לעזור לך להרגיש מעודכן, בטוח ובשליטה.
על ידי הרשמה אתה מקבל את שלנו מדיניות הפרטיות שלנו. באפשרותך לבטל את המנוי בכל עת. לעולם לא נמכור את הנתונים שלך.
עוד בניתוחים ופרוצדורות
- הרדמה
- הרדמה להחלפת ירך או ברך
- ארתרוסקופיה וניתוח ארתרוסקופי
- ביופסיה
- ביופסיה ושאיבת מח עצם
- הגדלת חזה
- הקטנת חזה
- אנגיופלסטיה כלילית
- מעקף עורקים כליליים
- שאיבת מחט טרנסברונכיאלית בהנחיית אולטרסאונד אנדוברונכיאלי
- הקלה בכאב באמצעות אפידורל לאחר ניתוח
- גסטרוסקופיה
- החלפת ירך
- החלפת ברך
- הסרת שיער בלייזר
- הרדמה מקומית לניתוח עיניים שלך
- ניתוח הקטנת אף (רינופלסטיקה)
- כאב ראש לאחר ניקור מותני
- זיהום חזה לאחר ניתוח
- הרדמה ספינלית